Author:
Australian Institute of Health and Welfare
Released:
27 February 2026
Cat. no:
GEN 015
Summary
The National Aged Care Data Asset (NACDA) brings together de-identified person-level data collected across aged care, health and community service settings for aged care research purposes.
The NACDA is an enduring asset, meaning data will be updated regularly and new tables and data sources added over time.
The purpose of this data resource profile is to provide information on scope, linkage rates and other data characteristics for researchers who want to access the NACDA.
The NACDA is available for both government and non-government researchers to access via the National Health Data Hub (NHDH). The key steps for NHDH access are:
- Eligibility – check the project aligns with eligibility requirements and approved uses for the NHDH.
- Ethics – most non-government projects require an additional Human Research Ethics Committee (HREC) approval (see NHDH frequently asked questions).
- Proposal – submit a project proposal to [email protected] (see NHDH Resources for template).
- Approval – AIHW facilitate approvals from the NHDH data custodian, the AIHW Ethics Committee delegate and the NHDH Advisory Committee.
- Onboarding – researchers complete NHDH onboarding training (conducted monthly) before they can access data through the secure access environment.
For more information, see NHDH researcher access, eligibility & costs.
Scope of linked aged care data
Aged care data available in the NACDA consists of over 80 tables covering key Australian government-funded aged care programs and assessments (see Data variable list for the NHDH). This includes home support, home care, residential care, flexible care and aged care eligibility assessments, with some data sources spanning 27 years.
The NACDA currently includes aged care data to 30 June 2024. In August 2026, the NACDA will be updated to incorporate aged care data to 30 June 2025 (Figure 1).
Figure 1: Scope of aged care data in the NACDA as at February 2026
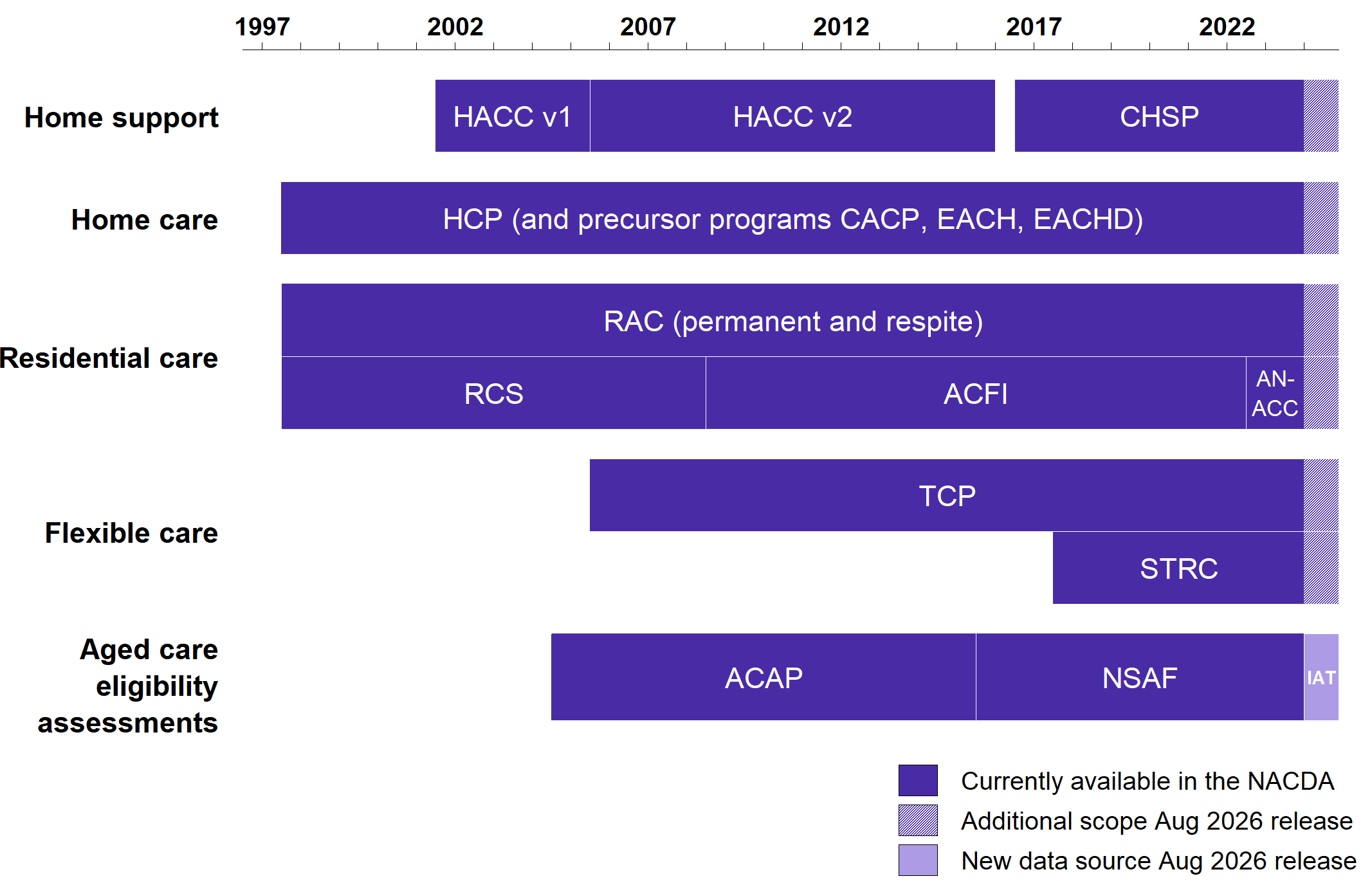
ACAP = Aged Care Assessment Program; ACFI = Aged Care Funding Instrument; AN-ACC = Australian National Aged Care Classification; CACP = Community Aged Care Program; CHSP = Commonwealth Home Support Program; EACH = Extended Aged Care at Home; EACHD = Extended Aged Care at Home Dementia; HACC = Home and Community Care; HCP = Home Care Packages [Program]; IAT = Integrated Assessment Tool; NSAF = National Screening and Assessment Form; RAC = residential aged care; RCS = Residential Classification Scale; STRC = Short-Term Restorative Care [Programme]; TCP = Transition Care Program.
Figure 1 is a graph that displays the approximate start and end dates for data in the NACDA for different aged care programs. The exact date ranges of aged care data modules in the NACDA are listed in Table 1.
Figure 1 also includes shaded areas for data that will be added to the NACDA in the August 2026 release:
- Data for all current aged care programs and assessments will be extended to include the period 1 July 2024 to 30 June 2025.
- Data for the Integrated Assessment Tool (IAT) will be added for the period 1 July 2024 to 30 June 2025.
Aged care data modules
Aged care data in the NACDA are largely administrative data generated as a by-product of the operation of aged care programs, and data collected from aged care assessments. The types of data available and the date range for each data module varies.
Table 1 describes the data available across the 8 aged care data modules in the NACDA. Two data modules – Home and Community Care, and Aged Care Assessment Program – contain data from historical programs which will not be updated in future releases. The National Screening Assessment Form is the largest of the current programs, with nearly 2.2 million people having a record in this data module.
Some aged care data modules contain multiple tables with different information. For example, the residential aged care data module includes separate tables on episodes of care, leave from care, details on care level, and care needs (funding) assessments. ‘By exception’ tables containing sensitive data items, such as full dates, and ‘conditional access’ tables containing specific data items that cannot be accessed alongside hospitals data, can also be requested where required for a project.
For more information on aged data modules in the NACDA and a complete list of data items, see Data variable list for the NHDH.
Table 1: Aged care data modules available in the NACDA as at February 2026
Care type |
Data module (aged care program) |
Data structure description |
Temporal range |
Number of people with data in module(a) |
| Home support | Home and Community Care (HACC) | Quarterly summary of service occasions, including type of service |
1 July 2001 to 1 April 2005 (v1) 1 July 2005 to 1 April 2015 (v2) |
1,105,166 (v1) 2,397,433 (v2) |
| Home support | Commonwealth Home Support Program (CHSP) | Single instances of services, including type of service, provided on particular date/s | 1 July 2016 to 30 June 2024 | 1,940,622 |
| Home care | Home Care Packages (HCP) Program(b) | Periods of care with entry/exit dates | 1 July 1997 to 30 June 2024 | 853,979 |
| Residential care | Residential aged care (RAC) | Periods of care with entry/exit dates, including permanent and respite care, and periodic care needs (funding) assessments | 1 July 1997 to 30 June 2024 | 1,766,853 |
| Flexible care | Transition Care Program (TCP) | Periods of care with entry/exit dates | 1 October 2005 to 30 June 2024 | 280,746 |
| Flexible care | Short-Term Restorative Care (STRC) | Periods of care with entry/exit dates | 1 March 2017 to 30 June 2024 | 36,478 |
| Aged care eligibility assessments | Aged Care Assessment Program (ACAP) | Generally one-off eligibility assessment prior to care entry (comprehensive assessments only), including approvals and recommendations | 1 July 2004 to 30 June 2015 | 1,107,562 |
| Aged care eligibility assessments | National Screening and Assessment Form (NSAF) | Generally one-off eligibility assessment prior to care entry (home support and comprehensive assessments), including approvals and recommendations | 1 July 2015 to 30 June 2024 | 2,182,918 |
(a) Excludes people with unlinked records (i.e. data module records that did not link AIHW's Enhanced Medicare Spine).
(b) Includes precursor home care programs Community Aged Care Program (CACP), Extended Aged Care at Home (EACH) and Extended Aged Care at Home Dementia (EACHD).
Source: AIHW analysis of the National Aged Care Data Asset (February 2026).
Aged care data in the NACDA is updated annually. Data tables can change between releases due to ongoing aged care policy and program changes as well as feedback from NACDA users. Key changes to aged care tables from the 2024 (previous) to the 2025 (current) release included:
- Tables for all current programs were updated to include data to 30 June 2024 (previously 30 June 2022).
- Tables for historical (closed) programs were not updated but remain available (i.e. Home and Community Care, Aged Care Assessment Program).
- Residential aged care tables now include data back to 1 July 1997 (previously 1 July 2001).
- New table released (NAC_RAC_ANACC) containing funding assessment data from the Australian National Aged Care Classification in residential aged care (tool that replaced the Aged Care Funding Instrument in 2022).
- New table released (NAC_TCP_SETTING_DAYS) containing number of transition care days in a community or residential setting.
- New table released (NAC_HCP_RECIP_LOC) containing geography information for people receiving home care from 2020.
- Table removed (NAC_HCP_ASSESS) due to overlap with data from the National Screening and Assessment Form (NSAF).
- Common recipient and service tables across residential aged care, home care, short-term restorative care and transition care (NAC_AGED_RECIP and NAC_AGED_SVC) were split into separate tables for each program.
- Service tables for residential aged care, home care, short-term restorative care and transition care (tables ending in _SVC) now include history of characteristics as at 30 June for each year (previously latest record only).
- Recipient table for NSAF module (NAC_NSAF_RECIP) now includes change history for geography variables (previously latest record only).
- Recipient table for CHSP module (NAC_CHSP_RECIP) now includes history of characteristics as at 30 June for each year (previously latest record only).
Retained versions of aged care tables from the previous release are available to researchers in the NACDA (indicated by the release year suffix _YY).
Due to the above changes in temporal scope and other data revisions, counts in the last release differ slightly to those published in this release.
For more information on aged data tables in the NACDA and a complete list of data items, see Data variable list for the NHDH.
Where does the aged care data come from?
Aged care data in the NACDA are sourced from the National Aged Care Data Clearinghouse (NACDC), an independent and central repository of (unlinked) national aged care data.
The NACDC was established at the AIHW in 2013. The Australian Government Department of Health, Disability and Ageing supplies annual data extracts to the AIHW for the NACDC.
For more information, see National Aged Care Data Clearinghouse: User guide.
Characteristics of aged care recipients
The NACDA contains data on over 4.7 million Australians who used one or more government-funded aged care programs or received an aged care eligibility assessment between 1997 and 2024.
Use of multiple aged care programs
By linking person records from different aged care programs, the NACDA can be used to explore people’s pathways through the aged care system.
Table 2 outlines the proportion of people who have linked records across different aged care programs. For example, of the over 1.9 million people who used the Commonwealth Home Support Program, 26% are also recorded as having used the Home Care Packages Program at some point. By comparison, of the nearly 854,000 people who used the Home Care Packages Program, more than half (59%) are also recorded as having used the Commonwealth Home Support Program.
Table 2: People with linked records across selected aged care data modules in the NACDA as at February 2026
Program |
CHSP (%) |
HCP(a) (%) |
RAC (%) |
TCP (%) |
STRC (%) |
Number of people
|
| CHSP | - | 25.9 | 24.8 | 7.6 | 1.7 | 1,940,622 |
| HCP(a) | 58.9 | - | 52.6 | 12.5 | 3.0 | 853,979 |
| RAC | 27.2 | 25.4 | - | 9.5 | 0.5 | 1,766,853 |
| TCP | 52.6 | 38.0 | 59.7 | - | 0.8 | 280,746 |
| STRC | 91.8 | 70.5 | 23.4 | 6.4 | - | 36,478 |
CHSP = Commonwealth Home Support Program; HCP = Home Care Packages [Program]; RAC = residential aged care; STRC = Short-Term Restorative Care [Programme]; TCP = Transition Care Program.
(a) Includes precursor home care programs Community Aged Care Program (CACP), Extended Aged Care at Home (EACH) and Extended Aged Care at Home Dementia (EACHD).
Source: AIHW analysis of the National Aged Care Data Asset (February 2026).
Aged care use over time
The NACDA contains data back to 1997 for some aged care programs. This means trends in use of aged care services can be followed for up to 27 years, as well as health service use for these aged care recipients for the years where data is available.
Long term trends in aged care should be interpreted with consideration for changes in programs and policy over time. For example, a number of aged care reforms and changes were implemented between 2015 and 2017. This includes introduction of the Short-Term Restorative Care (STRC) program, rollout and expansion of the Commonwealth Home Support Program (CHSP), and changes to the Home Care Packages (HCP) Program.
New Aged Care Act
This page presents data up to the 2023–24 financial year, before the Aged Care Act 2024 came into effect on 1 November 2025. Changes since the commencement of the new Act and the beginning of the Support at Home program, alongside a new regulatory model, will be reported when data become available in the NACDA. For more information on the new Act, see New Aged Care Act on the Department of Health, Disability and Ageing website.
This page presents data up to the 2023–24 financial year, before the Aged Care Act 2024 came into effect on 1 November 2025. Changes since the commencement of the new Act and the beginning of the Support at Home program, alongside a new regulatory model, will be reported when data become available in the NACDA. For more information on the new Act, see New Aged Care Act on the Department of Health, Disability and Ageing website.
The number of people using different aged care programs in the NACDA varied over time (Figure 2 and Figure 3). The overall trend is that people are increasingly using community-based aged care programs like home support and home care.
- The number of people using home support increased from 642,000 in 2016–17 to 778,000 in 2023-24 (21% increase).
- The number of people using home care increased steadily from 5,600 in 1998 to 63,800 in 2016, and then nearly quadrupled between 2017 and 2024 (from 71,700 to 274,000).
- The number of people using residential care increased between 2001 and 2016 (103,000 to 186,000), remained relatively stable between 2017 and 2022 (188,000 to 190,000), and then increased again to 201,000 people in 2024.
Figure 2: People using aged care by care type and sex, between 30 June 1998 and 2024
Line chart shows the number of people using aged care (home support, home care, residential care, transition care and short-term restorative care) by sex between 30 June 1998 and 2024.
Figure 3: People using aged care by care type and age group, between 30 June 1998 and 2024
Line chart shows the number of people using aged care (home support, home care, residential care, transition care and short-term restorative care) by age group between 30 June 1998 and 2024.
The number of admissions per financial year in the NACDA also varied by aged care program over time (Figure 4). Admissions generally increased for home care, residential care and short-term restorative care, but admissions to transition care steadily decreased in the later years.
- The number of admissions to home care increased from 7,600 in 1997–98 to 42,800 in 2016–17, and then almost doubled between 2017–18 and 2023–24 (from 53,600 to 102,000), peaking in 2022–23 (121,000).
- The number of admissions to residential care increased from 1997–98 to 2016–17 (from 85,400 to 150,000), remained relatively stable between 2017–18 and 2021–22 (fluctuating between 150,000 and 154,000), and then increased again to 173,000 in 2023–24.
- The number of admissions to transition care increased from 6,800 in 2006–07 to 23,400 in 2012–13, remained relatively stable between 2013–14 and 2016–17 (fluctuating between 24,400 and 24,900), and then gradually decreased from 25,100 in 2017–18 to 14,300 in 2023–24.
- The number of admissions to short-term restorative care increased steadily since the introduction of the program in March 2017 – from 1,600 in 2017–18 to 9,100 in 2023–24.
Figure 4: Aged care admissions by care type and sex, between 1997–98 and 2023–24
Line chart shows the number of admissions to aged care services (home care, residential care, transition care and short-term restorative care) by sex between 1997–98 and 2023–24.
The aged care recipient data reported in this section are sourced from the NACDA and may differ from counts published elsewhere, based on unlinked data. Through the data linkage process, duplicate records belonging to a single person are more readily identified and accounted for in the analysis presented in this section.
For a comprehensive list of data items available for aged care recipients in the NACDA, see Data variable list for the NHDH.
Characteristics of aged care services
The NACDA holds rich information on people accessing aged care, but also contains de-identified information on aged care services and providers.
Expanding the availability of de-identified provider-level data is a priority for future development of NACDA (see Future expansion).
The number of aged care services (i.e. facilities or outlets that deliver aged care) in the NACDA varied by care type, organisation type and remoteness (Figure 5). This section reports on aged care services that have delivered home care, residential care, transition care or short-term restorative care between 1997 and 2024.
- More than half of aged care services were residential care facilities (51%), and 42% were home care services.
- Not-for-profit organisations operated nearly two-thirds of aged care services (64%), compared with private organisations (27%) and government organisations (9%).
- Nearly two-thirds of aged care services were in Major cities of Australia (63%), compared with 23% in Inner Regional Australia and 10% in Outer Regional Australia. Less than 4% of aged care services were located in Remote Australia and Very Remote Australia.
Figure 5: Aged care services by care type, organisation type and remoteness, 1997–2024
Bar charts show the total number of aged care services by care type, organisation type and remoteness for the period 1997 to 2024.
For a comprehensive list of data items available for aged care services in the NACDA, see Data variable list for the NHDH.
Quality of linked aged care data
Person-level data have been available for some aged care programs nationally since 1997. However, the information and payment systems collecting data for the different programs do not use a common person identifier, and so are not integrated at the source.
Data linkage brings together data from different information and payment systems.
Linkage process
Identifiers from each aged care program are individually linked to AIHW’s Enhanced Medicare Spine (EMS) to allow person-level data to be integrated across aged care programs, and with health and community services data.
The EMS covers the majority of the Australian population, as demonstrated by the high linkage rate achieved in linkages with national data sources (for example, see Table 3). The EMS is created by combining personal identifiers from the Medicare Consumer Directory (e.g. full name, date of birth) with information drawn from the National Death Index and the Australian Immunisation Register. The EMS is updated regularly.
Both probabilistic name-based linkage and multi-step key-based linkage methods are used for the NACDA, depending on the availability of personal identifiers for each aged care program.
Linkage rates
Table 3 outlines the number of records from the source data and linkage rates for each aged care data module in the NACDA.
All aged care programs using probabilistic name-based linkages had very high linkage rates (over 99.5%). Name-based linkage is used where full name and demographic information are available in the source data. This approach was used for home care, residential care, transition care, short-term restorative care and aged care eligibility assessments using the National Screening and Assessment Form.
The linkage rates for aged care programs using multi-step key-based linkages were lower. Key-based linkage is performed using a statistical linkage key (SLK-581), where full name and demographic information are not available in the source data. The Commonwealth Home Support Program had the lowest linkage rate (94.9%) of all the current (ongoing) aged care data modules in the NACDA. The other key-based linkages were for historical programs – Home and Community Care, and Aged Care Assessment Program – which will not be updated in future releases.
Table 3: Linked and unlinked records from source data for each aged care data module in the NACDA as at February 2026
Aged care data module |
Linkage type |
Linked records (%) |
Unlinked records (%) |
Number of records from source data(a) |
| Home and Community Care (HACC) v1 | key | 92.6 | 7.4 | 7,818,637 |
| Home and Community Care (HACC) v2 | key | 92.9 | 7.1 | 25,556,306 |
| Commonwealth Home Support Program (CHSP)(b) | key | 94.9 | 5.1 | 6,260,212 |
| Home Care Packages (HCP) Program(c) |
name | 99.7 | 0.3 | 856,152 |
Residential aged care (RAC) |
name | 99.5 | 0.5 | 1,774,893 |
| Transition Care Program (TCP) |
name | 99.7 | 0.3 | 349,725 |
| Short-Term Restorative Care (STRC) |
name | 99.9 | 0.1 | 36,511 |
| Aged Care Assessment Program (ACAP) |
key | 97.4 | 2.6 | 2,100,180 |
| National Screening and Assessment Form (NSAF) |
name | 99.7 | 0.3 | 2,461,350 |
(a) Source data may include duplicate records (i.e. duplicate identifiers) for the same individual. Therefore, the number of records from source data (Table 3) may not be equal to the number of people with data in module (Table 1 and Table 2) for a given aged care data module.
(b) The number of total records and percentage of linked records for the Commonwealth Home Support Program module has substantially increased from the previous release due to the recipient table for this program now containing multiple records per person.
(c) Includes precursor home care programs Community Aged Care Program (CACP), Extended Aged Care at Home (EACH) and Extended Aged Care at Home Dementia (EACHD).
Data item quality
Like all linked administrative data assets, data quality in the NACDA varies between data modules, individual tables and individual data items.
Linkage of multiple administrative data records mean there are multiple opportunities to ascertain important information about a person. It also means information can differ between data sources for the same person. Researchers can choose to use different statistical methods to resolve these inconsistencies and/or increase the ascertainment of characteristics that are known to be underreported in administrative data.
Table 4 outlines the differences between individual tables in the reporting of selected person demographic characteristics (sex and year of birth), focusing on Commonwealth Home Support Program (CHSP) and Home Care Packages (HCP) program recipients. Overall, inconsistencies between these tables are low. Over 97% of people have matching sex across the tables analysed, and similarly over 97% have matching year of birth.
Table 4: Comparison of demographic characteristics across NACDA tables as at February 2026
Characteristic |
NACDA tables compared |
Characteristic matches (%) |
Characteristic does not match (%) |
Number of people across tables |
| Sex | NAC_HCP_RECIP vs NAC_CHSP_RECIP | 97.5 | 2.5 | 518,526 |
| Sex | NAC_HCP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 99.9 | 0.1 | 869,667 |
| Sex | NAC_CHSP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 98.0 | 2.0 | 1,981,434 |
| Sex | NAC_HCP_RECIP vs NAC_CHSP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 97.5 | 2.5 | 518,526 |
| Year of birth | NAC_HCP_RECIP vs NAC_CHSP_RECIP | 98.4 | 1.6 | 518,526 |
| Year of birth | NAC_HCP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 98.3 | 1.7 | 869,667 |
| Year of birth | NAC_CHSP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 98.5 | 1.5 | 1,981,434 |
| Year of birth | NAC_HCP_RECIP vs NAC_CHSP_RECIP vs PATIENTS_DEMOGRAPHY_SEP25 | 97.8 | 2.2 | 518,526 |
Note: NAC_HCP_RECIP and NAC_CHSP_RECIP are NACDA tables containing recipient demographic information for the home care program and Commonwealth Home Support Program data modules (respectively). PATIENTS_DEMOGRAPHY_SEP25 is a NACDA demographics table for all people with a linked service event record in one or more of the National Health Data Hub content tables, with sex and year of birth based on the Medicare Consumer Directory. See Data tables for comparisons across additional modules.
Source: AIHW analysis of the National Aged Care Data Asset (February 2026).
For a description of data quality for individual data items in the NACDA, covering domains such as accuracy, validity and completeness, see Data variable list for the NHDH.
Scope of other linked data
Data in the NACDA are de-identified, meaning personally identifying information such as full name and full date of birth are removed. A unique person-number is used to follow individuals through the available data modules and across previously siloed systems.
The NACDA is accessible via AIHW’s National Health Data Hub (NHDH). As at February 2026, the NACDA via the NHDH contains de-identified data on key government-funded aged care programs and assessments, linked to prescription medicines, Medicare-subsidised services, immunisations, cancer screening and cancer diagnosis, hospitalisations, intensive care, National Disability Insurance Scheme (NDIS), and deaths data (Figure 6).
Figure 6: Data modules in the NACDA via the National Health Data Hub as at February 2026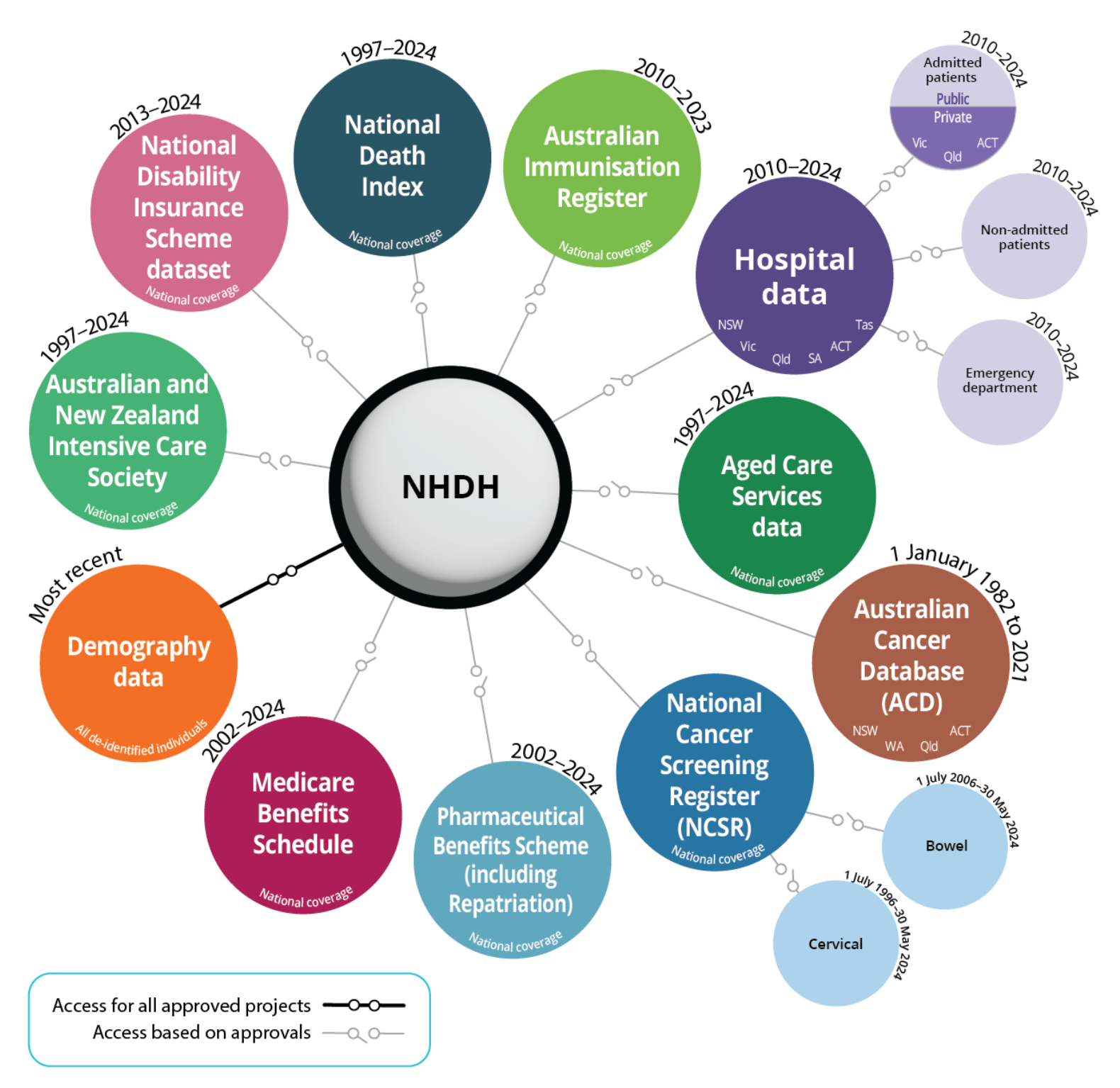
Source: National Health Data Hub.
Figure 6 is a diagram with 17 circles. At the centre is a circle that says NHDH. There is one circle connected which has 'access for all approved projects' called Demography data which contains all de-identified individuals and is marked as 'most recent'. The following are the other 11 circles around the central circle, representing those with 'access based on approval':
- 1997–2024: Aged Care Services data (national coverage)
- 2017–2024: National Disability Insurance Scheme data set (national coverage)
- 2010–2023: Australian Immunisation Register (national coverage)
- 2010–2024: Hospital data (NSW, Vic, Qld, SA, ACT, Tas)
- 2010–2024: Admitted patients (public | private – Vic, Qld, ACT)
- 2010–2024: Emergency department
- 2010–2024: Non-admitted patients
- 2010–2024: Medicare Benefits Schedule (national coverage)
- 1997–2024: National Death Index (national coverage)
- 2002–2024: Pharmaceutical Benefits Scheme – including Repatriation (national coverage)
- 2017–2024: Australian and New Zealand Intensive Care Society (national coverage)
For more information about data modules available in the NACDA via the NHDH, including future expansion, see NHDH Data & data items.
Future expansion
The NACDA was a recommendation of the Royal Commission into Aged Care Quality and Safety (Royal Commission) to ensure reliable and comprehensive data about the sector is available for research.
The AIHW is responsible for delivering the NACDA, in consultation with research, non-government, peak body and government stakeholders.
Future development of the NACDA will focus on expanding data sources to include de-identified provider-level aged care data on care quality, workforce and financials – as outlined by the Royal Commission. These data are expected to be available in the NACDA by the end of 2026.
For more information on aged care data expansion in the NACDA, see the NACDA webpage.
Where can I find out more?
More information about the National Aged Care Data Asset (NACDA) is available on the NACDA webpage.
How to access NACDA
The NACDA is available for both government and non-government researchers to access via the National Health Data Hub (NHDH). For more information, see NHDH researcher access, eligibility & costs.
Current NACDA projects
As at 12 January 2026, there were 34 active (fully approved) projects using the NACDA via the NHDH. For a list of active projects using the NACDA, visit the NACDA webpage. For a list of all NHDH projects, visit NHDH Approved projects and status.
Contact
For more information, contact the NACDA team at the AIHW through the enquiry form, via email at [email protected] or 02 6244 1000.
